|
A friend recommended using EuropePMC, https://europepmc.org/ as an alternative to PubMed (thank you, Chris). This repository describes themselves as:
Doing a search on EuropePMC is similar to doing a search on PubMed (which works much like a Google search; see this recent blog post), but the search results can be quite different. Hmm. Why?
- Europe PMC is an open science platform that enables access to a worldwide collection of life science publications and preprints from trusted sources around the globe.
- Europe PMC is developed by EMBL-EBI. It is a partner of PubMed Central and a repository of choice for many international science funders.
- Free, transparent, and community-driven, Europe PMC is your gateway to life science research.
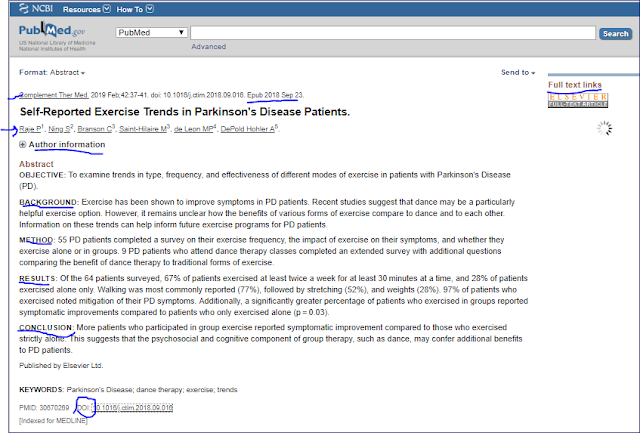
Many things are the same with PubMed and EuropePMC. There are Basic (like a Google search) and Advanced search available in both (for searches by journal, for example). You can also sort the results by date or by "relevance"/"best match." Further, you can limit results for a particular date range and whether there is a free article available for both, and you can search by article type, but each repository does it differently (advanced search in EuropePMC, filters in PubMed). The way the two identify free articles (full articles available to all) is a bit different, but both seem to have the same access. In addition, both have ways to tell about other research that cites this article (a real-world measure of influence), show links to similar articles, and highlight keywords. Here is an excerpt from a sample EuropePMC search:

The more restrictive your keywords are, the more similarities you find between the two tools. When I used the keywords (example: Parkinson's dementia rivastigmine) and sorted by recent date, the first article is the same - but many of the rest of the citations/abstracts are not.
But what causes the differences? Partly different journals are available (there are more in EuropePMC), but partly, I suspect, because of different indexing (selection of keywords for each article). Here's a recording of a webinar about how to do search on EuropePMC:
Another difference is that PubMed will let you email a search to yourself, which is handy if you use multiple computers; you can email just the citations in EuropePMC, but since EuropePMC saves your previous searches - and you can sign in to the system - the email may not be as important. Also, some features in filters on both platforms don't seem to work, but I can't tell if this is a limitation based on indexing that just hasn't been done.
I happen to prefer PubMed, probably because I'm used to it. But I use both repositories to search research. When I don't find results in one, I often can find results in the other (one of the reasons I suspect the indexing is different).
See which one you prefer.